

This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Breakthrough Chemotherapy Heart Protection Discovery for Zantrene
22 November 2021 – Race Oncology Limited (“Race”) is pleased to share interim results from the Zantrene® preclinical heart safety research program led by eminent cardiotoxicity researchers, Associate Professors Aaron Sverdlov and Doan Ngo, in collaboration with cancer scientist Associate Professor Nikki Verrills, at The University of Newcastle (ASX announcement: 28 April 2021).
This research has found that Zantrene is able to protect heart muscle cells from anthracycline (specifically doxorubicin) induced cell death while improving the killing of breast cancer cells.
Anthracyclines are one of the most effective anti-cancer treatments developed and are used in more cancer settings than any other class of chemotherapeutic agent1. These drugs are used to treat millions of cancer patients every year, including those with leukemias, lymphomas, neuroblastoma, kidney, liver, stomach, uterine, thyroid, ovarian, sarcomas, bladder, lung and breast cancers. The clinically most important anthracyclines are doxorubicin, daunorubicin, epirubicin and idarubicin2.
To date, the concept of potential cancer therapies that are not only non-cardiotoxic but, in fact, cardio-protective has not been evaluated or even entertained, largely due to ‘disease-specific’ approaches in healthcare. Our results suggest that Zantrene, an effective anti-cancer medication, can concomitantly provide protection against toxic effects on the heart from one of the most commonly used chemotherapy agents, doxorubicin. This is the first evidence of its kind to demonstrate that there is a therapy that both targets the cancer and protects the heart! This has the potential to improve health outcomes for countless cancer patients and survivors by both improving their cancer treatment while preventing development of cardiovascular disease.
Associate Professor Aaron Sverdlov
While highly effective anti-cancer drugs, the anthracyclines cause serious and permanent damage to the heart in many patients.
Zantrene® (bisantrene dihydrochloride) was originally developed as a heartsafer alternative to the anthracyclines particularly with respect to preservation of heart muscle3. While Zantrene’s improved heart safety was proven in more than 50 clinical trials4, , the question as to whether Zantrene could help prevent the heart damage caused by anthracyclines has never been addressed.
After the discovery that Zantrene is a potent FTO inhibitor, this is a second ‘once in a lifetime’ discovery. To find that Zantrene can protect the heart from chemotherapy while also killing cancers better is an extraordinary ‘best of both worlds’ outcome. Given anthracyclines are used in millions of cancer patients every year, it is hard to overstate the clinical and commercial potential of this breakthrough!
Chief Scientific Officer, Dr Daniel Tillett
Zantrene’s cardio toxic properties were always of interest, but this novel cardio protective insight is far more significant to the drug’s potential application as an adjunctive to anthracycline backbone chemotherapy. I look forward to the team quickly advancing these investigations so we might assess and progress this opportunity as a matter of substantial priority.
Chief Executive Officer, Mr Phillip Lynch
Study Background
Anthracycline Cardiotoxicity
Anthracyclines are highly effective anticancer agents, but their use in patients comes with a significant risk of permanent damage to the heart. Some studies have estimated that over half of patients exposed to anthracyclines will develop some form of heart disease within 6 years of treatment5.
Anthracyclines, such as doxorubicin and epirubicin, can lead to either acute or late onset cardiotoxicity. Acute toxicity is associated with increased inflammation and can lead to a pericarditis-myocarditis syndrome. Flaccid, dilative cardiomyopathy is the predominant form of late onset anthracycline cardiotoxicity and can occur months to years after anthracycline exposure6.
Although the mechanism for early and late onset anthracycline cardiotoxicity remains unclear, risk factors include increased cumulative anthracycline dose, concurrent mediastinal radiation, extremes of age, female gender, and pre-existing heart disease7.
Prevention of Anthracycline Cardiotoxicity
A number of potential cardio-protective techniques and therapies have been explored over the years, ranging from modified anthracycline preparations, anti-oxidants, free radical scavengers, renin-angiotensin-system antagonists, cardio-selective beta-blockers to statins. While many showed promise in animal studies, clinical studies rendered mixed results with many agents offering little or no cardio-protective benefit and/or compromising the cancer treatment7.
As a consequence, cardio-protective treatments are not routinely used in clinical oncology practice, andthere remains a great demand for new treatment options that can prevent today’s cancer patient from becoming tomorrow’s cardiac patient.
Anthracyclines & Breast Cancer
Breast cancer accounts for 30% of all new cancer diagnoses in women8. It is estimated in the US during 2021 there will be 281,550 new breast cancer diagnoses and more than 43,600 deaths9. The vast majority (94%) of new breast cancer patients present with early stage disease8.
Anthracyclines, agents such as doxorubicin and epirubicin, are routinely used for the management of breast cancer with follow-up taxane-based therapy.
Surprisingly, women diagnosed with early-stage breast cancer were found to be more likely to die from cardiovascular disease than from breast cancer. Cardiovascular disease is also the leading cause of death in women over 75 diagnosed with stage II breast cancer10.
The risk of cardiotoxic damage is so elevated in breast cancer patients that many oncologists have moved in recent years to using anthracycline-free treatment regimens or limiting patient dosages, despite the well-established efficacy of anthracyclines11. As a result, many patients may receive sub-optimal cancer treatment, so potentially increasing their risk of cancer relapse and mortality.
In the late 1980s, Zantrene was the subject of a US based Phase 3 single agent clinical trial in advanced breast cancer patients. This Phase 3 trial showed that Zantrene had comparable efficacy to standard of care treatment, doxorubicin, but was associated with significantly less damage to the patients’ hearts. Some 23% of patients who received doxorubicin suffered serious heart failure compared to just 4% with Zantrene12.
Study Highlights
1. Zantrene protects cardiomyocytes from doxorubicin-induced cell death
The laboratory study found Zantrene was able to protect or rescue primary human heart muscle (cardiomyocyte) cells from doxorubicin-induced cell death. Incubation of cardiomyocytes in the presence of 1000 nM doxorubicin for 72 hours resulted in 80% cell death (Fig. 1). Protection from cardiomyocyte cell death was observed upon the inclusion of 250 nM Zantrene and increased further with higher concentrations, reaching 60% survival (3-fold increase) at 5000 nM. At 1000 nM of Zantrene, cardiomyocyte survival was greater than 48%, a concentation that is less than 15% of the in vivo maximium achieved and tolerated dose in humans13.
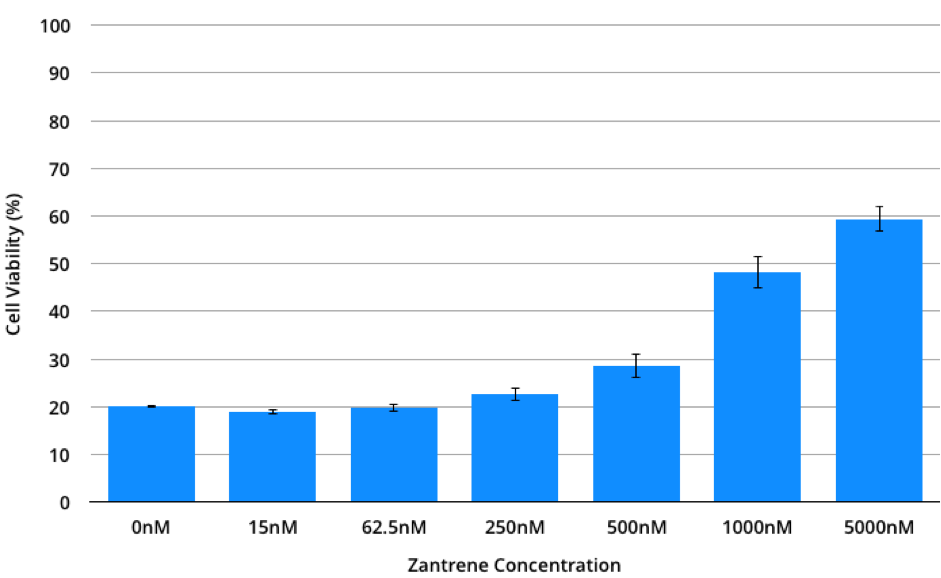
Figure 1. Primary human cardiomyocyte cell viability when cultured in the presence of 0-5000 nM of Zantrene and 1000 nM doxorubicin for 72 hours. Data is the average of eight full replicates, each performed in triplicate. Bars show the standard error.
2. Zantrene synergises with doxorubicin and epirubicin to better kill breast cancer cells
Previous studies have found Zantrene synergises with the breast cancer chemotherapy drug, cyclophosphamide (ASX Announcement: 9 March 2021). This study was extended to examine synergy between Zantrene and doxorubicin or Zantrene and epirubicin. Inclusion of even lower levels of Zantrene (sub-125 nM) resulted in significant breast cancer cell death in the presence of doxorubicin or epirubicin (Table 1). This synergy was not limited to MB-231 as similar results were seen using MCF7 breast cancer cells which showed high levels of resistance to doxorubicin and epirubicin (ASX Announcement: 9 March 2021).
Table 1. MB-231 breast cancer cell viability (%) when cultivated in the presence of increasing concentration of Zantrene and doxorubicin (upper) or Zantrene and epirubicin (lower). Red shows drug combinations which result in high cell killing.
| Doxorubicin (nM) | ||||||
| Zantrene (nM) | 0 | 4 | 8 | 15 | 31 | 62.5 |
| 0 | 100.00 | 87.89 | 77.94 | 60.76 | 48.26 | 39.86 |
| 15 | 86.49 | 74.15 | 63.49 | 50.40 | 42.95 | 38.00 |
| 31 | 66.58 | 57.29 | 54.44 | 46.37 | 40.61 | 34.61 |
| 62.5 | 43.50 | 39.39 | 38.70 | 34.94 | 30.75 | 24.59 |
| 125 | 17.73 | 16.68 | 17.32 | 14.72 | 12.69 | 13.21 |
| 250 | 11.98 | 9.59 | 10.31 | 8.25 | 7.23 | 6.70 |
| Epirubicin (nM) | ||||||
| Zantrene (nM) | 0 | 4 | 8 | 15 | 31 | 62.5 |
| 0 | 100.00 | 86.10 | 76.47 | 55.97 | 45.39 | 38.97 |
| 15 | 91.63 | 74.19 | 62.01 | 52.12 | 38.31 | 37.11 |
| 31 | 62.57 | 51.21 | 48.08 | 39.19 | 34.44 | 31.76 |
| 62.5 | 43.21 | 35.12 | 32.56 | 28.58 | 24.81 | 21.28 |
| 125 | 15.96 | 13.77 | 13.11 | 11.29 | 9.86 | 7.99 |
| 250 | 12.01 | 9.15 | 8.25 | 8.06 | 5.56 | 5.64 |
Bliss Synergy Analysis17 showed a synergistic effect for both Zantrene and doxorubicin and Zantrene and epirubicin combinations in MB-231 breast cancer cells (Figs. 2 & 3). Similar results were also seen with MCF7 breast cancer cells (data not shown).
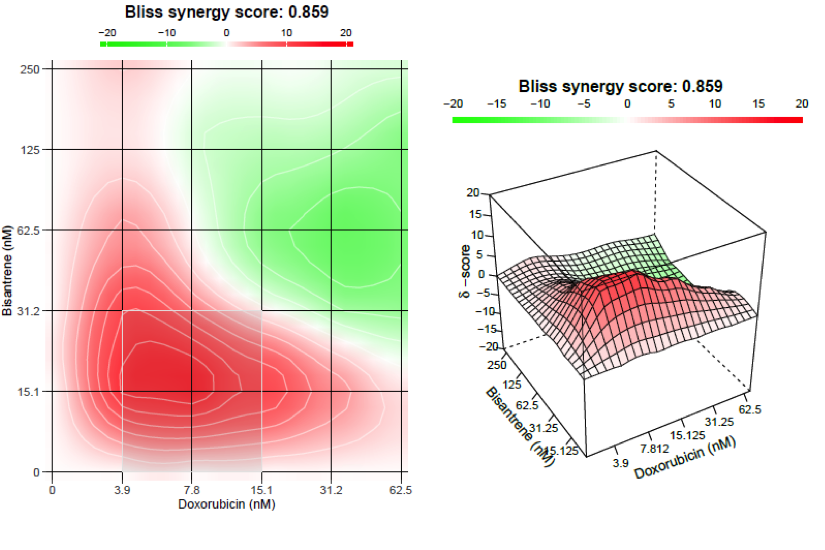
Figure 2. Bliss Synergy Analysis for MDA-MB-231 breast cancer cells treated with Zantrene and doxorubicin. Red to green scale indicating areas of synergy to antagonism. Values >10 are synergistic (red); values below -10 are antagonistic; values between -10 to 10 are additive. The most synergistic 2×2 area is indicated with a white box.
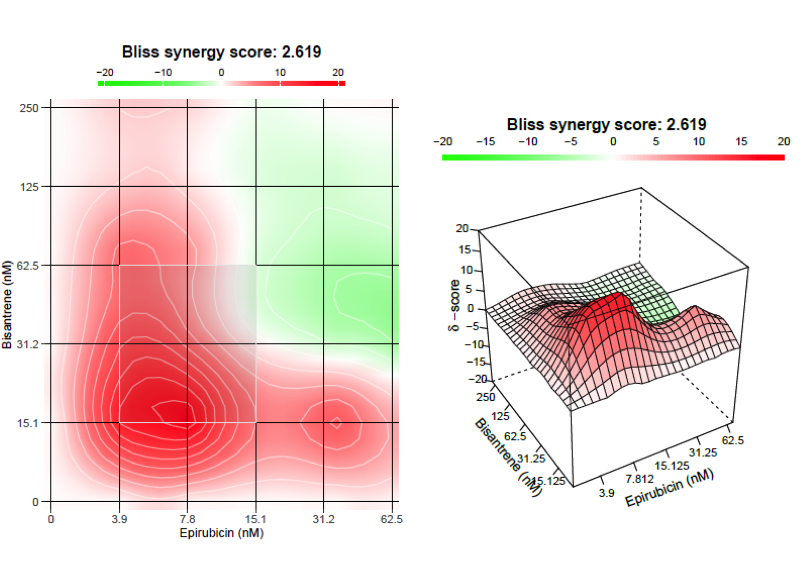
Figure 3. Bliss Synergy Analysis for MDA-MB-231 breast cancer cells treated with Zantrene and epirubicin. Red to green scale indicating areas of synergy to antagonism. Values >10 are synergistic (red); values below -10 are antagonistic; values between -10 to 10 are additive. The most synergistic 2×2 area is indicated with a white box.
Webb analysis16 showed additive synergy between Zantrene and doxorubicin and Zantrene and epirubicin over three different dose ranges (Fig. 4). At all drug concentrations and ratios, the combinations of Zantrene and doxorubicin or Zantrene and epirubicin were superior to either drug on its own.
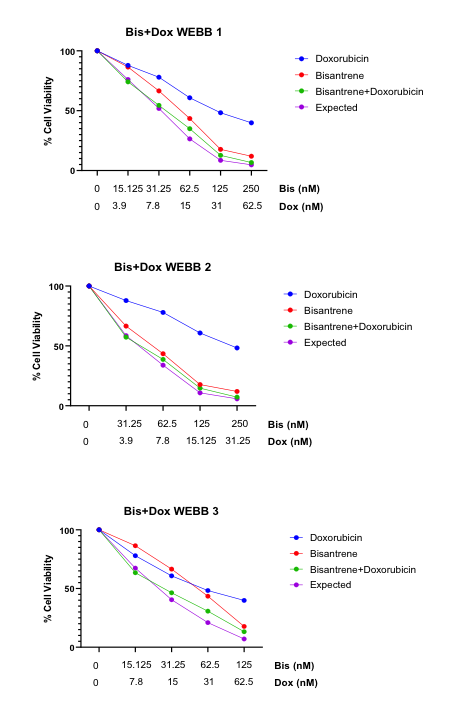
Figure 4. Webb analysis of MB-231 breast cancer cells treated with Zantrene and doxorubicin. Experimental data is shown for each drug alone and the combinations. The ‘Expected value’ is calculated using the method of Webb and represents the expected % cell viability if the drug combination is additive.
3. Cardio-protective mechanism of Zantrene is independent of FTO inhibition
The cardio-protective mechanism of Zantrene appears to be independent of its ability to effectively inhibit FTO14. Doxorubicin-induced cardiomycocyte cell death was not rescued by either of the other known FTO inhibitors, brequinar14 or FB23-215 (Figs. 5 & 6), suggesting Zantrene is acting via a novel cellular mechanism.
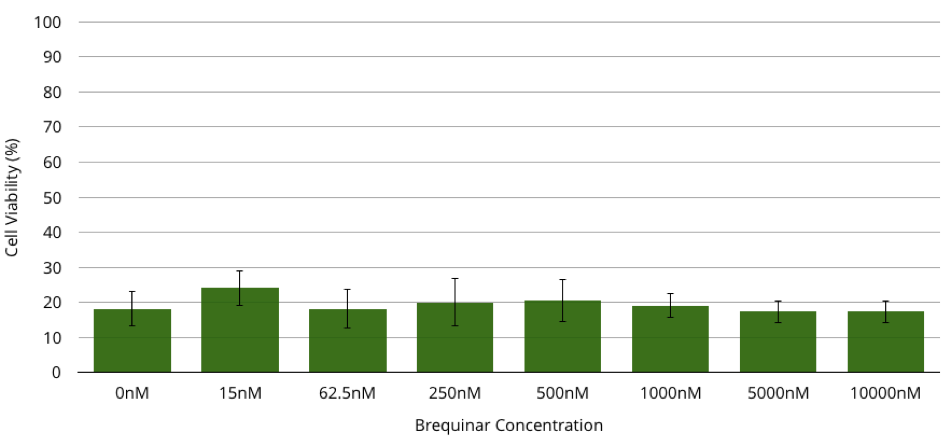
Figure 5. Primary human cardiomyocyte cell viability when cultured in the presence of 0-10000 nM of the FTO inhibitor brequinar and 1000 nM doxorubicin for 72 hours. Data represents the average of three full replicates, each performed in triplicate. Bars show the standard error.
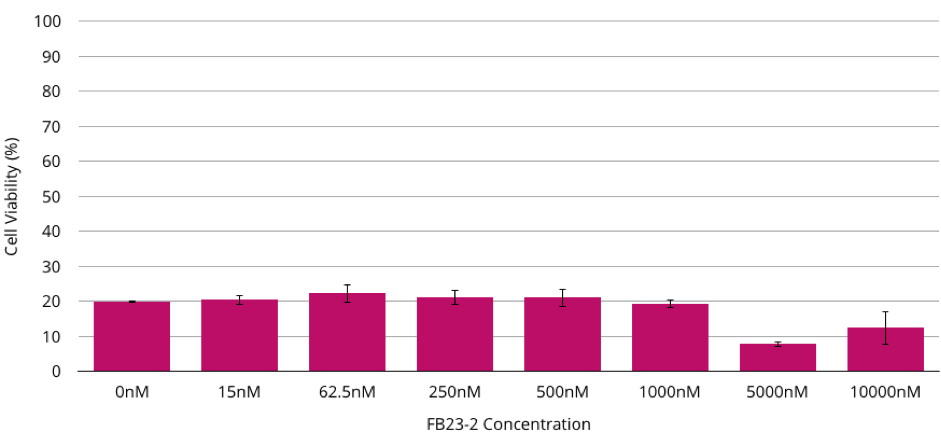
Figure 6. Primary human cardiomyocyte cell viability when cultured in the presence of 0-10000nM of the FTO inhibitor FB23-2 and 1000 nM doxorubicin for 72 hours. Data is the average of three full replicates, each performed in triplicate. Bars show the standard error.
Conclusions
- In this preclinical model, Zantrene protects the heart muscle cells from damage by doxorubicin while synergising with the anthracyclines to better kill breast cancer cells.
- Race has submitted a patent application addressing the combination of Zantrene with an anthracycline for the protection of the heart of patients. This patent (if granted) would provide protection of the drug combination and its clinical use through 2041.
- This new heart protection discovery will be rapidly progressed to the clinic. The extensive clinical history of Zantrene allows this combination to be quickly advanced clinically.
- Advanced discussions are underway with clinicians in Australia to run a Phase 2b clinical trial in breast cancer patients at serious risk of anthracycline-induced heart damage.
- This discovery opens new market opportunities for Zantrene of similar clinical and commercial potential to the earlier discovery that Zantrene is a potent FTO inhibitor.
Next Steps
- Animal studies to be run in Q4 CY2021/ Q1CY2022.
- Additional preclinical studies to investigate if Zantrene can protect the heart from damage by other chemotherapeutic drugs which are also known to cause cardio-damage.
- Further studies to determine the molecular mechanism of Zantrene’s cardio-protective activity. This may allow identification of additional protective functions of Zantrene.
- Development of new and optimised drug combination formulations with improved clinical and commercial value.
- Initiation of a Phase 2b breast cancer clinical trial in 2022.
Q&A
What do these cardio-protective results mean for Race?
While these are preclinical results, if the same results are repeated in patients, they would offer a completely new and unprecedented option for the clinical use of Zantrene. Previous research had identified Zantrene was a heart safer alternative to the effective yet cardiotoxic anthracyclines, and Zantrene was a potent inhibitor of the FTO m6A RNA demethylase, but its ability to prevent damage to the heart by the anthracyclines was unknown.
Race now has a new and compelling market opportunity that could be used to protect and better treat the millions of cancer patients that receive anthracycline chemotherapy every year.
It should be noted that reduced cardiac damage from Zantrene has been noted in more than 1500 patients in over 60 clinical trials. The heart damage seen in patients after exposure to anthracyclines is well recognized and has been replicated in multiple cell culture studies.
Have you obtained IP protection for these cardio-protection discoveries?
Yes. A patent application has been filed on this discovery which, if granted, would provide IP protection through 2041.
What is the market potential of this discovery?
This is difficult to answer beyond stating that millions of patients are treated every year with multiple cycles of anthracyclines and most are at risk of serious and permanent damage to their hearts. Fears over the damaging side effects of anthracyclines has led many oncologists to limit their use of these extremely effective drugs. This discovery has the potential to revolutionise the use of anthracyclines in the clinic by allowing oncologists to use these powerful drugs to their full anti-cancer potential without fear of permanent damage to the heart.
When can investors expect the next update?
We expect to be able to update our investors from late Q4 CY2021 on our further progress.
References
- 1. Weiss RB. The anthracyclines: will we ever find a better doxorubicin? Semin Oncol. (1992) 9(6):670-86.
- 2. Venkatesh P, Kasi A. Anthracyclines. (2021) In: StatPearls. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538187/
- 3. Citarella, R. V. et al. Activity of a novel anthracenyl bishydrazone, 9,10-anthracenedicarboxyaldehydeBis[(4,5-dihydro-1H-imidazol-2-yl)hydrazone] dihydrochloride, against experimental tumors in mice. (1982) Cancer Res 42, 440–4.
- 4. Rothman, J. The Rediscovery of Bisantrene: A Review of the Literature. (2017) Int J Cancer Res Ther 2, 1–10.
- 5. Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: a retrospective analysis of three trials. (2003) Cancer 97:2869–79.
- 6. Cai, F. et al. Anthracycline-induced cardiotoxicity in the chemotherapy treatment of breast cancer: Preventive strategies and treatment. (2019) Mol Clin Oncol 11, 15–23.
- 7. McGowan, J. V. et al. Anthracycline Chemotherapy and Cardiotoxicity. (2017) Cardiovascular drugs and therapy 31, 63–75.
- 8. Kimmick, G., Dent, S. & Klem, I. Risk of Cardiomyopathy in Breast Cancer: How Can We Attenuate the Risk of Heart Failure from Anthracyclines and Anti-HER2 Therapies? (2019)Curr Treat Options Cardiovasc Medicine 21, 30.
- 9. https://www.breastcancer.org/symptoms/understand_bc/statistics.
- 10. Waks AG, Winer EP. Breast cancer treatment: a review. (2019) JAMA. 321(3):288–300.
- 11. Ding, W. et al. Anthracycline versus nonanthracycline adjuvant therapy for early breast cancer: A systematic review and meta-analysis. (2018) Medicine 97, e12908.
- 12. Cowan, J. D. et al. Randomized Trial of Doxorubicin, Bisantrene, and Miltoxantrone in Advanced Breast Cancer: A Southwest Oncology Group Study. (1991) J National Cancer Inst 83, 1077–1084.
- 13. Alberts, D. S., Mackel, C., Pocelinko, R. & Salmon, S. E. Phase I clinical investigation of 9,10-anthracenedicarboxaldehyde bis[(4,5-dihydro-1H-imidazol-2-yl)hydrazone] dihydrochloride with correlative in vitro human tumor clonogenic assay. (1982) Cancer Res 42, 1170–5.
- 14. Su, R. et al. Targeting FTO Suppresses Cancer Stem Cell Maintenance and Immune Evasion. (2020) Cancer Cell 38, 79-96.e11.
- 15. Huang, Y. et al. Small-Molecule Targeting of Oncogenic FTO Demethylase in Acute Myeloid Leukemia. (2019) Cancer Cell 35, 677-691.e10 (2019).
- 16. Webb, J., Effect of more than one inhibitor In: Hochster ER, Quastel J (eds). Enzymes and metabolic inhibitors. (1963) Academic Press: New York. pp 487-512. 17. Bliss, C.I., The toxicity of poisons applied jointly. Ann. App. Biol, 1939. 26: p. 585-615.