

This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Expanded Heart Protection Discovery for Zantrene
08 December 2021 – Race Oncology Limited (“Race”) is pleased to share additional interim results from the Zantrene® (bisantrene dihydrochloride) preclinical heart safety research program led by eminent cardiotoxicity researchers, Associate Professors Aaron Sverdlov and Doan Ngo, in collaboration with cancer scientist Associate Professor Nikki Verrills, at The University of Newcastle (ASX announcement: 28 April 2021).
This research has found that Zantrene is able to also protect heart muscle cells from a new class of anti-cancer drug (carfilzomib) induced cell death while improving the carfilzomib-mediated killing of cancer cells.
Carfilzomib (trademark Kyprolis®) is a highly effective anti-cancer drug used in the treatment of multiple myeloma (a dangerous blood cancer), but it can cause serious and permanent damage to the heart in many patient1. The risk of cardiac damage is so great that its use in older patients with pre-existing heart disease is often contraindicated2.
“Carfilzomib is a highly effective anti-cancer drug, but it’s use is limited due to cardiotoxicity. Our laboratory has tested numerous drug candidates over the years, we observe that Zantrene has: 1. potent anti-cancer effects; 2. synergistic anti-cancer effects with both carfilzomib and doxorubicin; and 3. cardioprotective effects against both carfilzomib and doxorubicin-induced cardiotoxicity. Zantrene was shown to salvage over 30% of carfilzomib-induced human heart cell from death. These results are genuinely remarkable, as with other clinically used cardioprotective drugs, we only observe a 10-15% protection from heart cell damage.
Zantrene is the first anti-cancer agent that we have found to exhibit a cardioprotective profile while being synergistically effective as an anti-cancer treatment. These results give hope to the millions of patients living with cancer that once they survive cancer, they may not have to live with heart disease.”
Associate Professor Doan Ngo
While Zantrene’s improved heart safety compared to anthracyclines was demonstrated in more than 50 human clinical trial3,4, and has been shown in preclinical studies to protect heart muscle cells from anthracycline-induced death (ASX Announcement: 22 November 2021), the question as to whether Zantrene could help prevent cardiac damage caused by other classes of heart damaging cancer drugs had not been addressed.
“The expansion of Zantrene’s cardio-protection and anti-cancer synergy beyond the anthracyclines into the completely new drug class of proteasome inhibitors is unexpected. This discovery opens new clinical development pathways and partnering opportunities for Zantrene beyond those already identified by Race.”
CSO Dr Daniel Tillett
“This additional result further underscores the potential patient utility and commercial applicability for Zantrene. We will be allocating additional resources to ensure this discovery can be comprehensively addressed.”
Chief Executive Officer, Mr Phillip Lynch
Study Background
Multiple Myeloma
Multiple myeloma is dangerous leukaemia caused by the uncontrolled proliferation of the plasma white blood cells. It usually occurs in people aged over 60 and is more common in men. Multiple myeloma accounts for 10% of all blood cancers and is responsible for 1.8% of all new cancer cases in the United States, with a lifetime risk of 0.8% and a 5-year survival of 55.6% in 20215.
Carfilzomib mechanism of action and use
Carfilzomib is an intravenous drug for treating multiple myeloma in patients with relapsed or refractory disease after at least one previous therapy. It is given in combination with dexamethasone or with lenalidomide and dexamethasone6.
Originally developed by Proteolix before being acquired by Onyx Pharmaceuticals in 2009, carfilzomib is currently owned by Amgen after their acquisition of Onyx in 20137. Carfilzomib’s patent protection is expected to expire in 2025.
Carfilzomib is a 20S proteasome inhibitor that works by interfering with the system for breaking down proteins within cells. One of the hallmarks of cancer is the loss of control of normal protein synthesis and an increase in misfolded and damaged proteins that need to be removed. Inhibition of the 20S proteasome prevents these damaged proteins from being degraded, ultimately resulting in death of the cancer cells8.
Carfilzomib is administered to multiple myeloma patients in 28-day cycles. An intravenous infusion is given on two consecutive days each week for three weeks followed by a 12-day rest period. The annual cost of carfilzomib for a multiple myeloma patient is over US$300,000, with many patients treated for two or more years9.
Carfilzomib-induced cardiotoxicity
While effective in treating multiple myeloma, carfilzomib comes with significant risk of permanent heart damage. An analysis of the Phase 2 carfilzomib studies found of the 526 patients treated, 22% (n=116) of patients developed cardiac side-effects, 13.3% (n=70) showed arrhythmia, mainly atrial fibrillation, 7.2% (n=38) exhibited heart failure, 2% (n=9) developed treatment-associated cardiomyopathy, and 3% (n=18) suffered from ischemic heart disease2. Most cardiovascular events occurred early, with the first few doses administered10.
A history of atrial fibrillation/flutter or heart failure was more prevalent in patients experiencing cardiovascular events, emphasizing the importance of closely monitoring patients given carfilzomib11. Ionising radiation of the chest and/or anthracycline treatment also increases the risk of carfilzomib-induced cardiotoxicity, while biomarkers and echocardiography are not able to identify the patients most at risk for cardiovascular events12.
Study Highlights
1. Zantrene protects cardiomyocytes from carfilzomib-induced cell death
This study found Zantrene was able to protect or rescue primary human heart muscle (cardiomyocyte) cells from carfilzomib-induced cell death. Incubation of cardiomyocytes in the presence of 1000 nM carfilzomib for 72 hours resulted in 80% cell death (Fig. 2). Protection from cardiomyocyte cell death was observed upon the addition of 250 nM Zantrene and increased further with higher concentrations, reaching 50% survival (2.5-fold increase) at 1000 nM, a concentation that is less than 15% of the maximium achievable and tolerated dose in humans13.
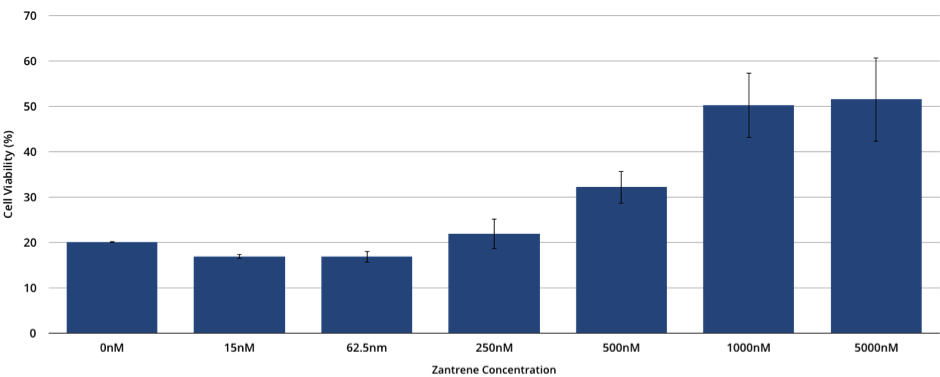
Figure 2. Primary human cardiomyocyte cell viability when cultured in the presence of 0-5000 nM of Zantrene and 1000 nM carfilzomib for 72 hours. Data is the average of five independent replicates, each performed in triplicate. Bars show the standard error.
2. Zantrene is highly active in killing multiple myeloma cancer cells
Zantrene was found to be highly active in killing the multiple myeloma cell line H929, with an IC50 below 15 nM (Fig. 3). Addition of only 10 nM carfilzomib to 15 nM of Zantrene resulted in 100% cell death (data not shown). Experiments are currently underway to determine the optimal synergistic combinations of these two drugs in multiple myeloma cell lines.
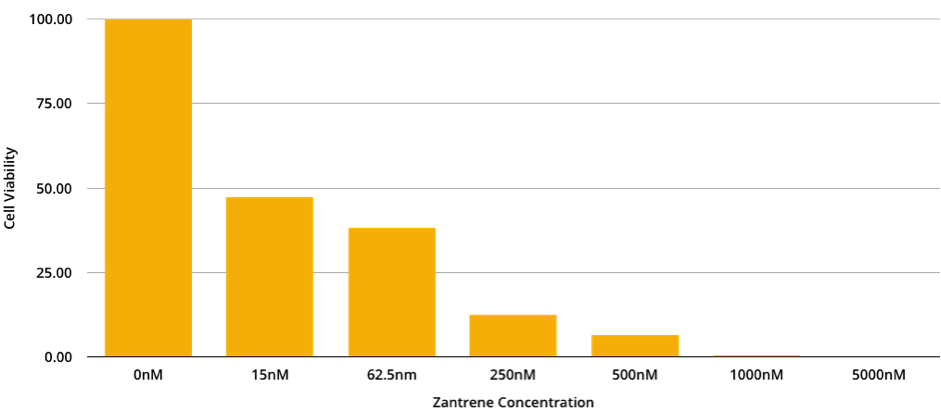
Figure 3. H929 Multiple Myeloma cell viability when cultured in the presence of 0-5000 nM of Zantrene for 72 hours.
3. Zantrene synergises with carfilzomib to better kill breast cancer cells
While carfilzomib has shown preclinical promise as a treatment for solid tumours including breast cancer, it has proven too toxic in patients to be used in the clinic8. This study examined potential synergy between Zantrene and carfilzomib. Inclusion of low concentrations of Zantrene (< 125 nM) resulted in significant breast cancer cell death in the presence of low concentrations of carfilzomib (Table 1). This synergy was not limited to the MB-231 cell line as similar results were seen using MCF7 cells (data not shown).
Table 1. MB-231 breast cancer cell viability (%) when cultured in the presence of increasing concentrations of Zantrene and carfilzomib. Red shows drug combinations that result in high cell killing.
| Carfilzomib (nM) | ||||||
| Zantrene (nM) | 0 | 0.625 | 1.25 | 2.5 | 5 | 10 |
| 0 | 100.00 | 95.83 | 85.92 | 67.92 | 25.80 | 1.56 |
| 15 | 89.34 | 82.57 | 72.93 | 57.97 | 24.51 | 2.90 |
| 31 | 71.60 | 61.96 | 59.14 | 50.69 | 25.96 | 3.87 |
| 62.5 | 49.55 | 46.78 | 40.56 | 37.15 | 22.14 | 3.77 |
| 125 | 28.10 | 26.29 | 24.74 | 24.71 | 17.68 | 1.90 |
| 250 | 22.76 | 22.72 | 23.53 | 23.07 | 7.74 | 0.00 |
Bliss Synergy Analysis14 revealed synergism between Zantrene and carfilzomib (Fig. 4). Similar results were seen with MCF7 breast cancer cells (data not shown).
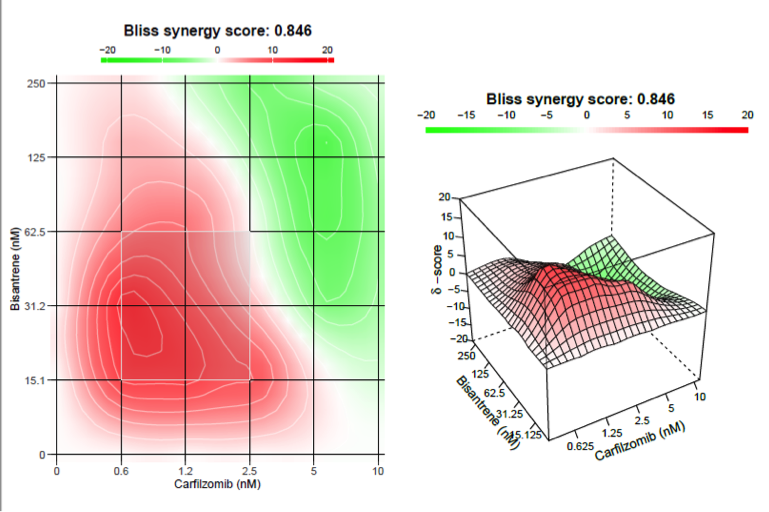
Figure 4. Bliss Synergy Analysis for MDA-MB-231 breast cancer cells treated with Zantrene and carfilzomib. Red to green scale indicating areas of synergy to antagonism. Values >10 are synergistic (red); values below -10 are antagonistic; values between -10 to 10 are additive. The most synergistic 2×2 area is highlighted with a white box.
4. Cardio-protective mechanism of Zantrene is independent of FTO inhibition
The cardio-protective mechanism of Zantrene appears to be independent of its ability to inhibit FTO16. Dac51, a recently developed potent FTO inhibitor with an IC50 of 400 nM17, was not able to protect cardiomyocytes from either doxorubicin-induced (Fig. 5) nor carfilzomib-induced cell death (Fig. 6). This finding is consistent with the previous observation that FTO inhibitors FB23-2 and brequinar do not protect against doxorubicin-induced cardiomyocyte cell death (ASX Announcement: 22 November 2021).
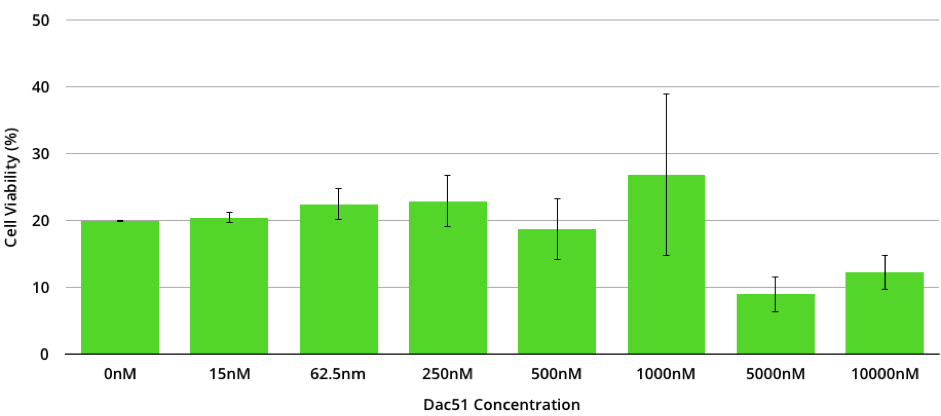
Figure 5. Primary human cardiomyocyte cell viability when cultured in the presence of 0-10000 nM of the FTO inhibitor Dac51 and 1000 nM doxorubicin for 72 hours. Data represents the average of three full replicates, each performed in triplicate. Bars show the standard error.
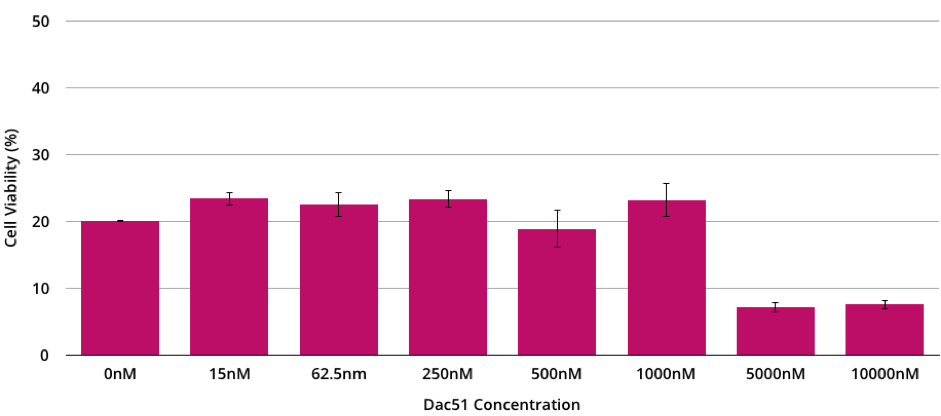
Figure 6. Primary human cardiomyocyte cell viability when cultured in the presence of 0-10000 nM of the FTO inhibitor Dac51 and 1000 nM carfilzomib for 72 hours. Data represents the average of three full replicates, each performed in triplicate. Bars show the standard error.
Conclusions
- In this preclinical study, Zantrene was shown to protect heart muscle cells from damage by carfilzomib while synergising to better kill breast cancer cells.
- This additional discovery suggests that Zantrene may be able to protect the heart of patients from a range of unrelated cardiac-damaging drugs.
- The synergy of Zantrene with carfilzomib in breast cancer cells may open the possibility of using carfilzomib in solid tumours, extending its potential to cancers beyond multiple myeloma.
- Race has submitted a patent application addressing the combination of Zantrene with carfilzomib for the protection of the heart of cancer patients. This patent (if granted) would provide protection of the drug combination and its clinical use through 2041.
- This new heart protection discovery can be rapidly progressed to the clinic. The extensive clinical history of Zantrene allows this combination to be quickly advanced clinically in multiple myeloma.
- This discovery opens new collaboration potential and licensing opportunities for Zantrene.
Next Steps
- Animal studies to be conducted in Q1-Q2 CY2022.
- Additional preclinical studies to investigate if Zantrene can protect the heart from damage by other chemotherapeutic drugs that are also known to cause cardio-damage.
- Further studies to determine the molecular mechanism of Zantrene’s cardio-protective activity. This may allow identification of additional protective functions of Zantrene.
- Development of new and optimised drug combination formulations with improved clinical and commercial value.
Q&A
What do these additional cardio-protective results mean for Race?
While these are preclinical results, if the same results are repeated in patients, they would offer a completely new and unprecedented option for the clinical use of Zantrene. Previous research had identified Zantrene as a heart-safer alternative to the effective yet cardiotoxic anthracyclines and as a potent inhibitor of the m6A RNA demethylase FTO, but its ability to prevent damage to the heart by the anthracyclines – and now carfilzomib – was unknown.
It should be noted that reduced cardiac damage from Zantrene has been noted in more than 1500 patients in over 60 clinical trials. The heart damage seen in patients after exposure to carfilzomib is well recognized and has been replicated in multiple cell culture studies as well as animal studies.
Have you obtained IP protection for these cardio-protection discoveries?
Yes. A patent application has been filed on this discovery which, if granted, would provide IP protection through 2041.
What is the market potential of this discovery?
This is difficult to answer beyond stating that many cancer types are sensitive to 20S proteasome inhibitors like carfilzomib.
When does the patent on carfilzomib expire and what would this discovery mean to the current owner of carfilzomib?
Carfilzomib is owned by Amgen and their patent expires in 2025. A reformulation of carfilzomib with Zantrene may offer a way of extending the patent life of carfilzomib beyond 2025.
When can investors expect the next update?
We expect to be able to update our investors from early Q2 CY2022 on our further preclinical progress with regards to this program. Any potential discussion with pharma partners will be announced when appropriate.
References
1. Ito, S. Proteasome Inhibitors for the Treatment of Multiple Myeloma. (2020) Cancers 12, 265.
2. Heckmann, M. B., Doroudgar, S., Katus, H. A. & Lehmann, L. H. Cardiovascular adverse events in multiple myeloma patients. (2018) J Thorac Dis 1, S4296–S4305.
3. Citarella, R. V. et al. Activity of a novel anthracenyl bishydrazone, 9,10-anthracenedicarboxyaldehydeBis[(4,5-dihydro-1H-imidazol-2-yl)hydrazone] dihydrochloride, against experimental tumors in mice. (1982) Cancer Res 42, 440–4.
4. Rothman, J. The Rediscovery of Bisantrene: A Review of the Literature. (2017) Int J Cancer Res Ther 2, 1–10.
5. https://seer.cancer.gov/statfacts/html/mulmy.html
6. Manasanch, E. E. & Orlowski, R. Z. Proteasome inhibitors in cancer therapy. (2017) Nat Rev Clin Oncol 14, 417–433.
7. https://investors.amgen.com/news-releases/news-release-details/amgen-acquire-onyx-pharmaceuticals-125-share-cash
8. Sherman, D. J. & Li, J. Proteasome Inhibitors: Harnessing Proteostasis to Combat Disease. (2020) Molecules 25, 671.
9. Roy, A. et al. Estimating the Costs of Therapy in Patients with Relapsed and/or Refractory Multiple Myeloma: A Model Framework. (2015) Am Heal Drug Benefits 8, 204–15.
10. Siegel D, Martin T, Nooka A, et al. Integrated safety profile of single-agent carfilzomib: experience from 526 patients enrolled in 4 phase II clinical studies. (2013) Haematologica 98:1753-61.
11. Chen JH, Lenihan DJ, Phillips SE, et al. Cardiac events during treatment with proteasome inhibitor therapy for multiple myeloma. Cardio-Oncology 2017;3:4.
12. Rosenthal A, Luthi J, Belohlavek M, et al. Carfilzomib and the cardiorenal system in myeloma: an endothelial effect? (2016) Blood Cancer J 6:e384.
13. Alberts, D. S., Mackel, C., Pocelinko, R. & Salmon, S. E. Phase I clinical investigation of 9,10-anthracenedicarboxaldehyde bis[(4,5-dihydro-1H-imidazol-2-yl)hydrazone] dihydrochloride with correlative in vitro human tumor clonogenic assay. (1982) Cancer Res 42, 1170–5.
14. Bliss, C.I., The toxicity of poisons applied jointly. (1939). Ann. App. Biol,. 26: p. 585-615.
15. Webb, J., Effect of more than one inhibitor In: Hochster ER, Quastel J (eds). Enzymes and metabolic inhibitors. (1963) Academic Press: New York. pp 487-512.
16. Su, R. et al. Targeting FTO Suppresses Cancer Stem Cell Maintenance and Immune Evasion. (2020) Cancer Cell 38, 79-96.e11.
17. Liu, Y. et al. Tumors exploit FTO-mediated regulation of glycolytic metabolism to evade immune surveillance. (2021) Cell metabolism 33, 1221-1233.e11.